
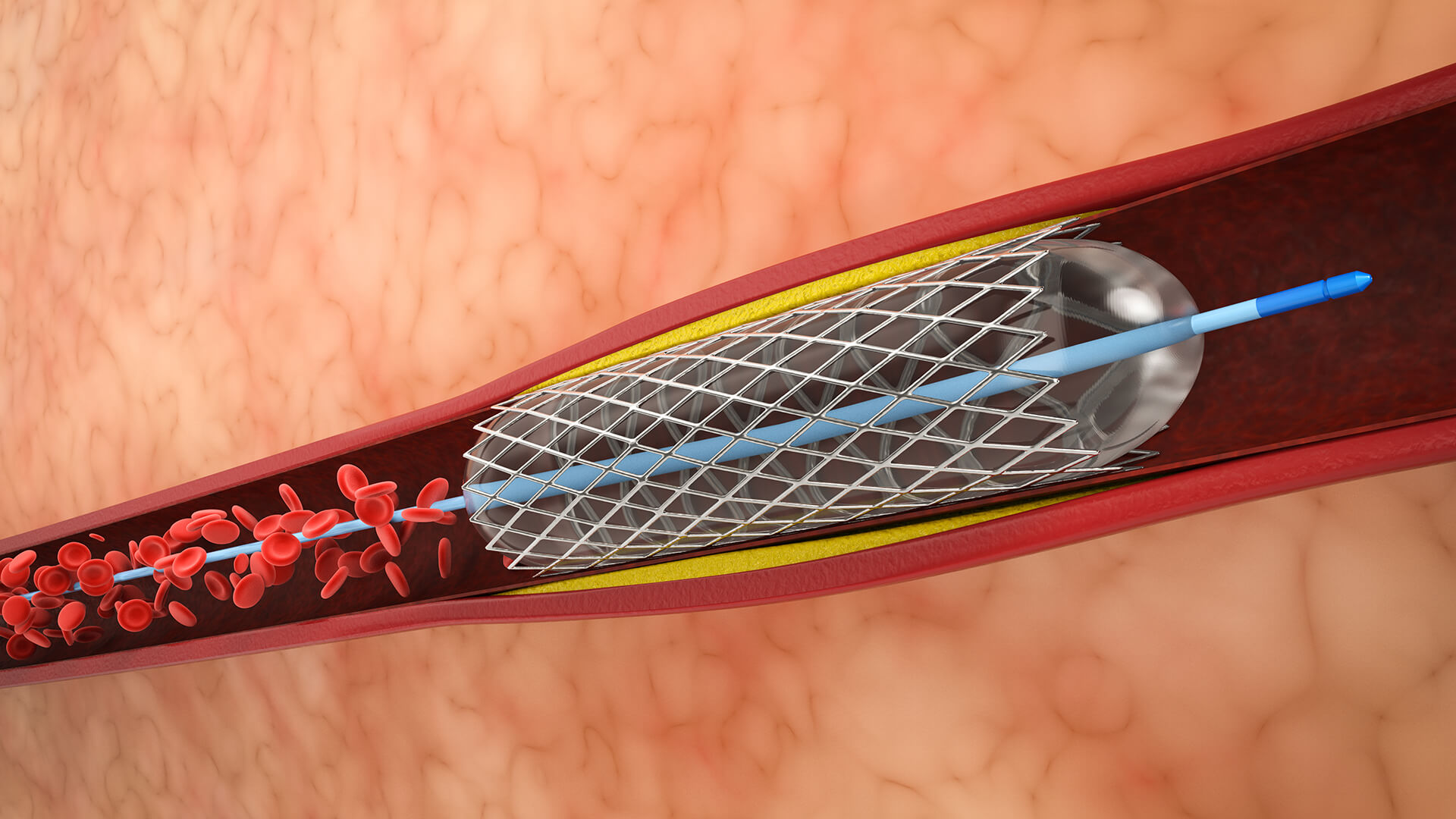
1. Vascular Access and Configuration
Obtain vascular access, usually through the femoral artery. In the parent artery that supplies the aneurysm, place a guiding catheter proximally.

Lorem Ipsum is simply dummy text of the printing and typesetting industry.

Lorem Ipsum is simply dummy text of the printing and typesetting industry.

















