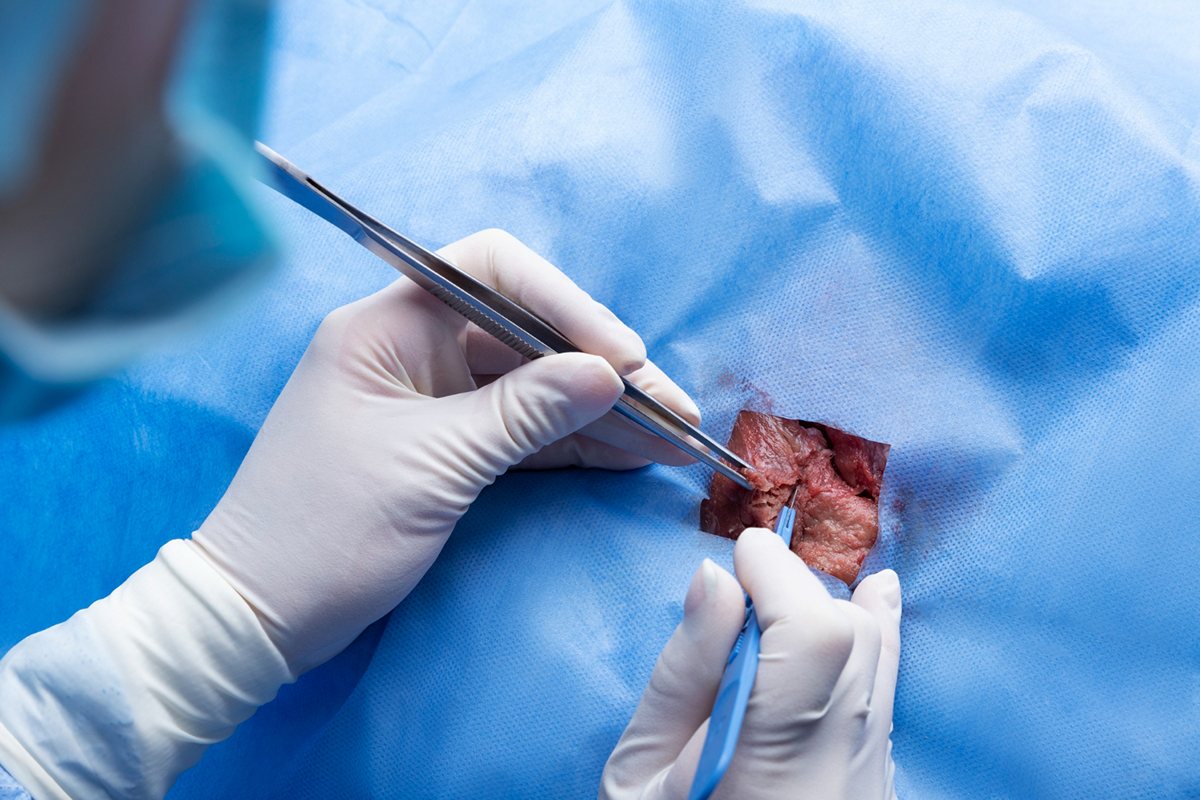
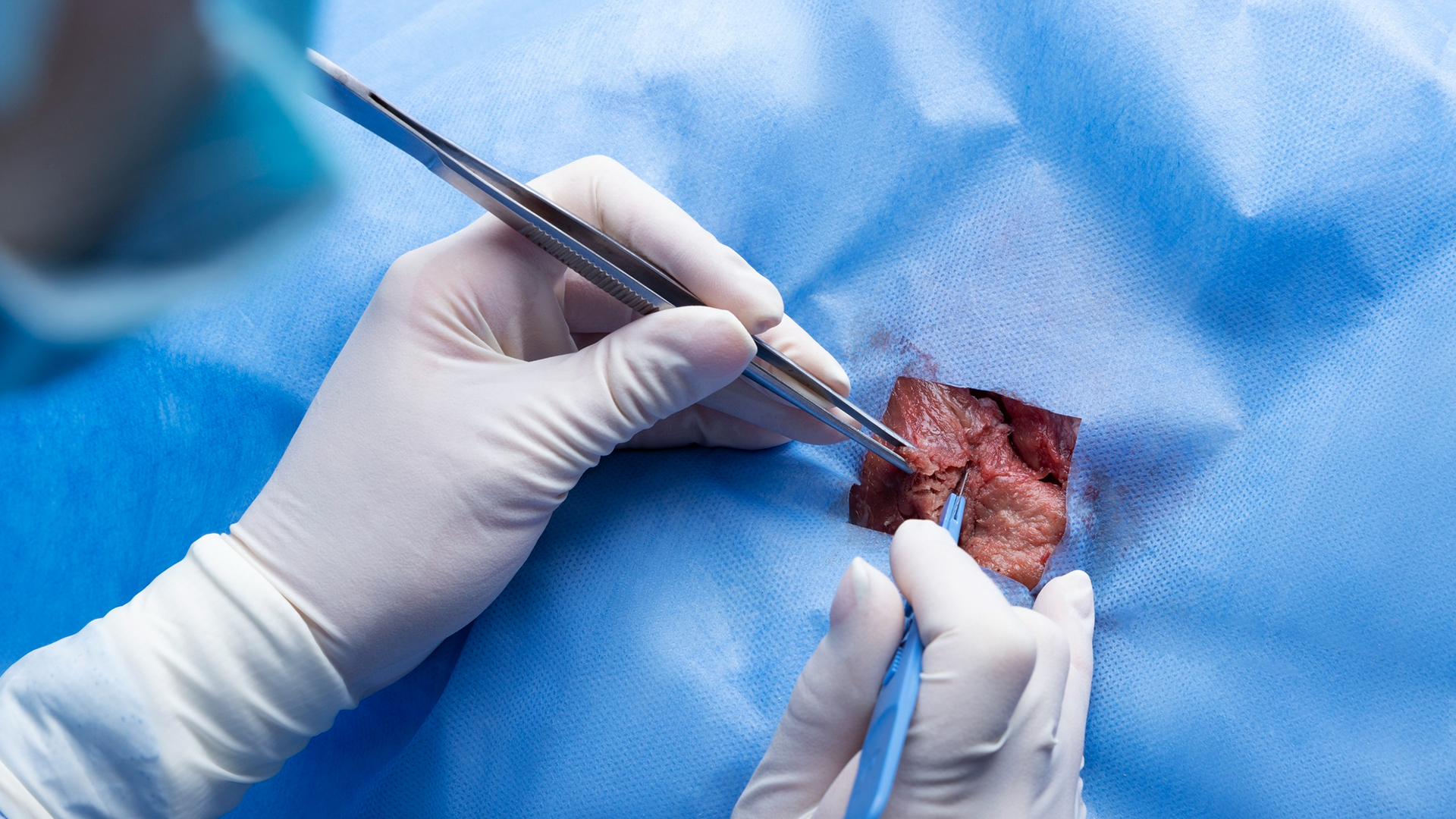
1. Setting Up and Positioning
Usually in a comfortable position, the patient lies down. Depending on how visible the lesion is, ultrasonography, mammography, or MRI guidance are used to pinpoint its location.

Lorem Ipsum is simply dummy text of the printing and typesetting industry.