
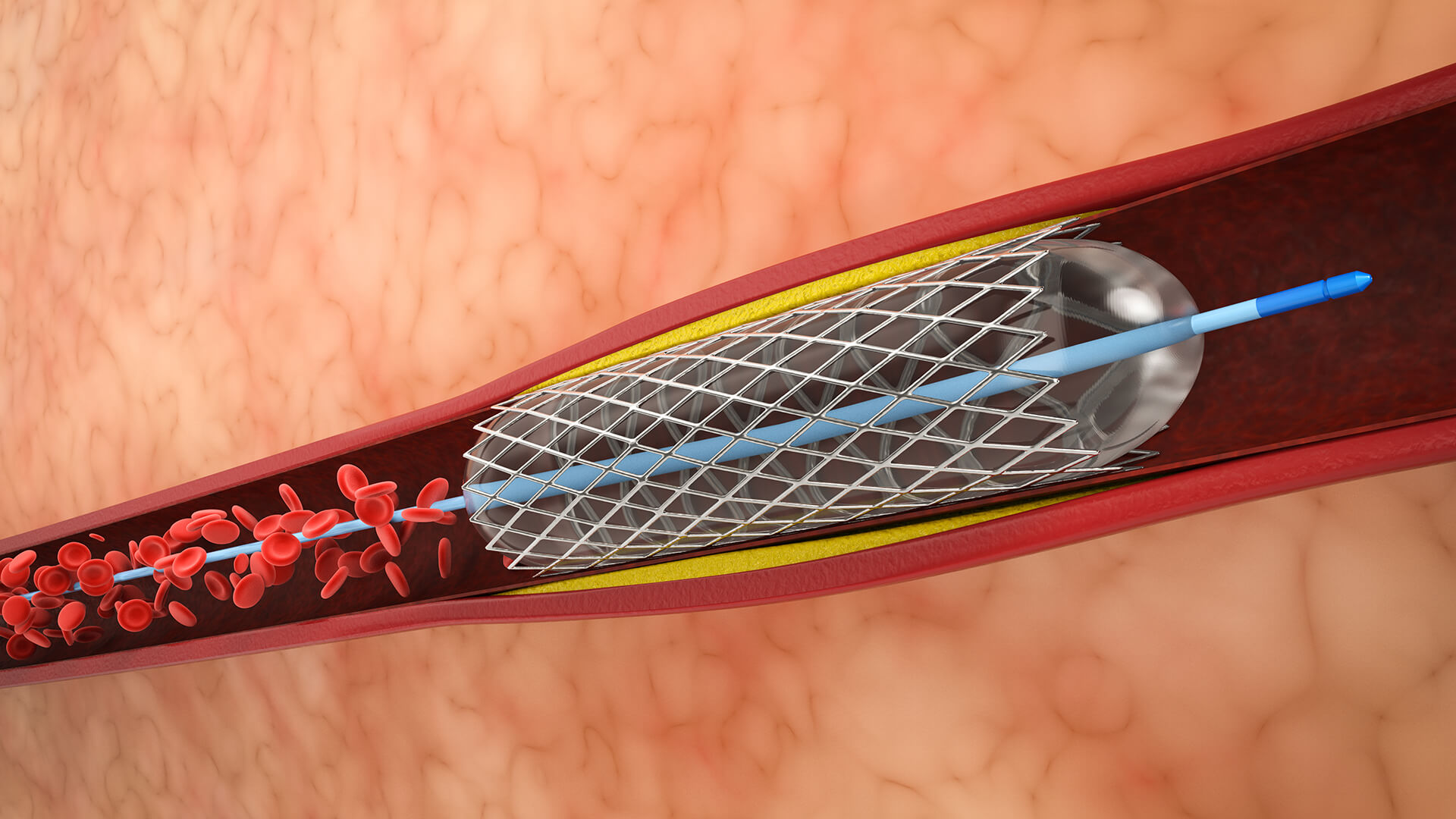
1. Placement of Catheters and Vascular Access
Usually, the femoral artery is used to get access. A guiding catheter is inserted close to the aneurysm in the parent artery.

Lorem Ipsum is simply dummy text of the printing and typesetting industry.

Lorem Ipsum is simply dummy text of the printing and typesetting industry.

Lorem Ipsum is simply dummy text of the printing and typesetting industry.
















