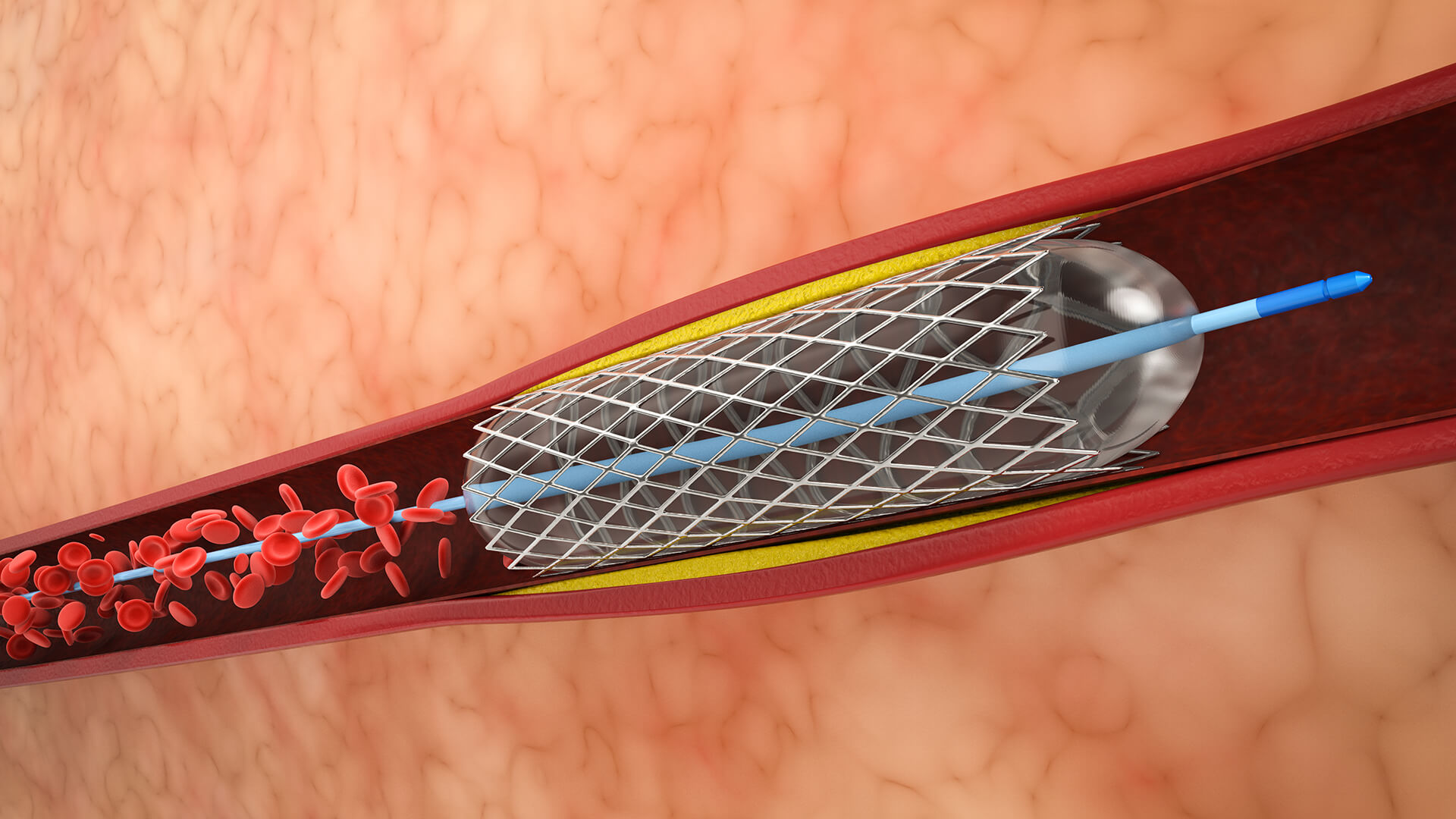
1. Getting Ready and Getting Access
In a sterile setting, the patient is positioned and prepared. The access site, typically the wrist or groin is where local anesthetic is given. To introduce a vascular sheath, a little incision is made.

Lorem Ipsum is simply dummy text of the printing and typesetting industry.

Lorem Ipsum is simply dummy text of the printing and typesetting industry.

Lorem Ipsum is simply dummy text of the printing and typesetting industry.