1. Preparation and Assessment
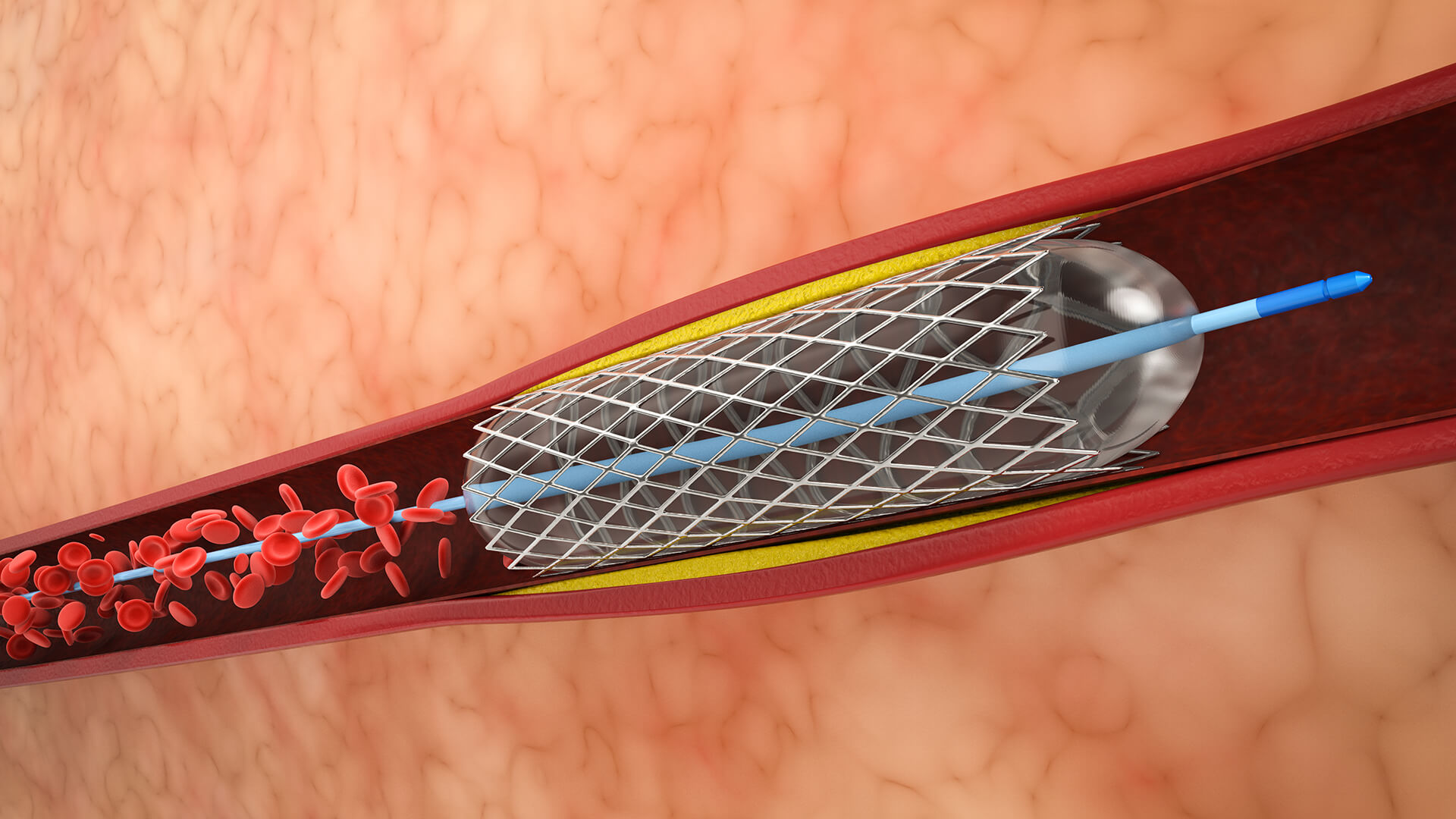
To determine arterial blockages and appropriateness, the patient gets a pre-procedure evaluation that includes blood tests, an ECG, and angiography.

Lorem Ipsum is simply dummy text of the printing and typesetting industry.

Lorem Ipsum is simply dummy text of the printing and typesetting industry.

Lorem Ipsum is simply dummy text of the printing and typesetting industry.