Pelvic Congestion Syndrome

Pelvic Congestion Syndrome

The pelvic pain and discomfort may progressively worsen, becoming chronic and significantly impacting the quality of life.
Symptoms like backache, abnormal and heavy menstrual bleeding, and painful intercourse can intensify.
Varicose veins around the vulva, thighs, and pelvic region may become more prominent and painful.
Women may experience increased urinary frequency, abnormal vaginal discharge, fatigue, and depression due to ongoing pain and discomfort.
The pain may eventually become persistent, occurring even at rest, and can interfere with daily activities and emotional well-being.
Untreated PCS can lead to chronic pelvic pain that is difficult to manage and may require more invasive treatments later on.

diagnosis
Lorem Ipsum is simply dummy text of the printing and typesetting industry. Lorem Ipsum has been the industry's standard dummy text. Lorem Ipsum is simply dummy text of the printing and typesetting industry

Clinical history and physical examination
-
 Tenderness over ovarian points on pelvic exam and persistent pelvic pain that lasts longer than six months and gets worse when standing or having sex may raise suspicions. There may be visible varicose veins in the upper legs or vulva.
Tenderness over ovarian points on pelvic exam and persistent pelvic pain that lasts longer than six months and gets worse when standing or having sex may raise suspicions. There may be visible varicose veins in the upper legs or vulva.

Pelvic ultrasound with Doppler
-
First-line noninvasive imaging for detecting venous reflux, visualizing dilated and tortuous pelvic veins, and ruling out other causes of pelvic pain is pelvic ultrasound (transabdominal and transvaginal) with Doppler. Valsalva or positional changes during ultrasonography are examples of dynamic maneuvers that improve reflux detection. The diagnosis is supported by slow or reversed blood flow and an ovarian vein diameter greater than 6 mm.
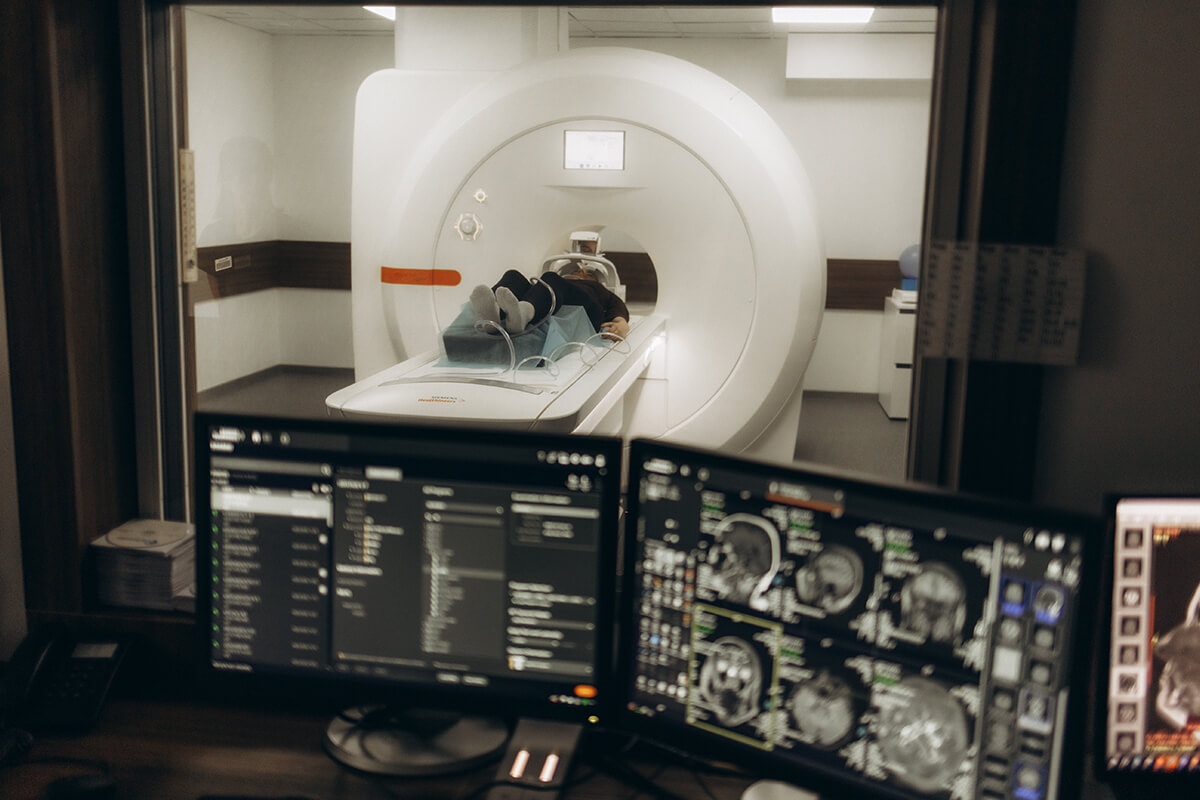
MRI and Magnetic Resonance Venography (MRV)
-
Pelvic veins and varicosities can be seen anatomically in great detail with magnetic resonance imaging (MRI) and magnetic resonance venography (MRV). Although specialized venous protocols for MRI are effective, patient positioning may limit their use.

CT scan
-
Due to radiation, computed tomography (CT) scans are less common in premenopausal women, although they can confirm venous insufficiency and show pelvic varices.

Ovarian and iliac venography
-
Known as pelvic venography, is regarded as the gold standard for diagnosis. To view venous anatomy and identify dilatation, reflux, and pelvic varicosities, a catheter is placed into the pelvic veins and contrast dye is injected. If necessary, this invasive test also permits concurrent therapeutic embolization.

Laparoscopy
-
Sometimes used to rule out other causes of persistent pelvic pain, such as endometriosis, laparoscopy frequently misses PCS because of positioning and insufflation effects that conceal pelvic varices.