Pain From Metastatic Lesions

Pain From Metastatic Lesions

Severe, persistent pain: Pain may worsen, become incessant, and refractory to simple analgesics, severely impacting quality of life.
Pathological fractures: Weakened bones are prone to fractures, causing sudden, severe pain and physical disability.
Spinal cord compression: Metastases to the vertebrae can compress the spinal cord or nerve roots, leading to neurological deficits such as paralysis, loss of bladder/bowel control, numbness, and weakness.
Hypercalcemia of malignancy: Excess bone breakdown releases calcium into the bloodstream, causing nausea, vomiting, constipation, confusion, fatigue, cardiac arrhythmias, and coma if untreated.
Anemia and marrow suppression: Bone marrow infiltration by tumor can reduce red blood cell production causing anemia, fatigue, and increased infection risk.
Reduced mobility: Pain and skeletal complications reduce function and independence.
Psychosocial impact: Chronic pain and disability can lead to depression, anxiety, and reduced social participation.

diagnosis
Lorem Ipsum is simply dummy text of the printing and typesetting industry. Lorem Ipsum has been the industry's standard dummy text. Lorem Ipsum is simply dummy text of the printing and typesetting industry

Clinical Evaluation
-
 Assess patient history including known malignancy and symptoms like localized bone pain, fractures, or neurological signs from nerve compression.
Assess patient history including known malignancy and symptoms like localized bone pain, fractures, or neurological signs from nerve compression.

X-rays
-
Initial screening tool to identify osteolytic or osteoblastic lesions and detect pathological fractures. Limited sensitivity for small lesions.
Bone Scintigraphy (Bone Scan)
-
Uses radionuclide tracer (99mTc-MDP) to detect areas of increased bone activity indicating metastases. High sensitivity but less specific.

Computed Tomography (CT)
-
Provides detailed assessment of bone cortex destruction and lesion morphology, useful for surgical planning.
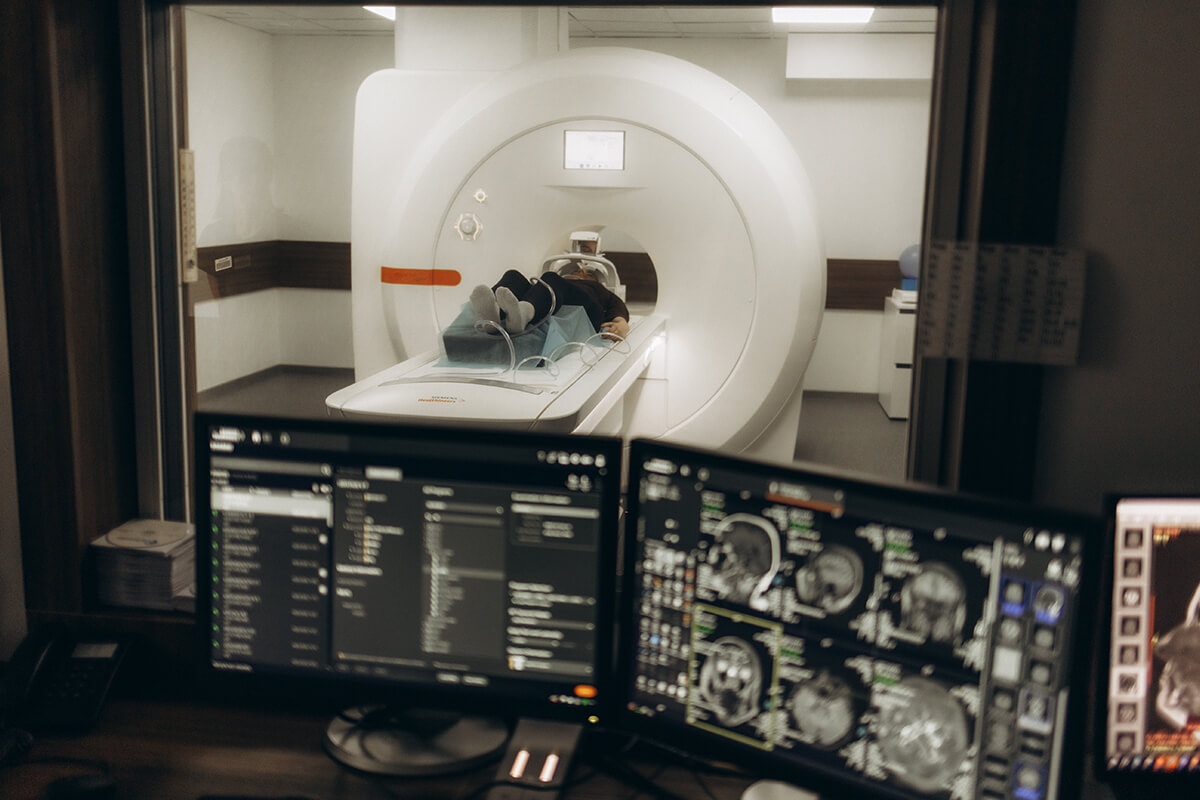
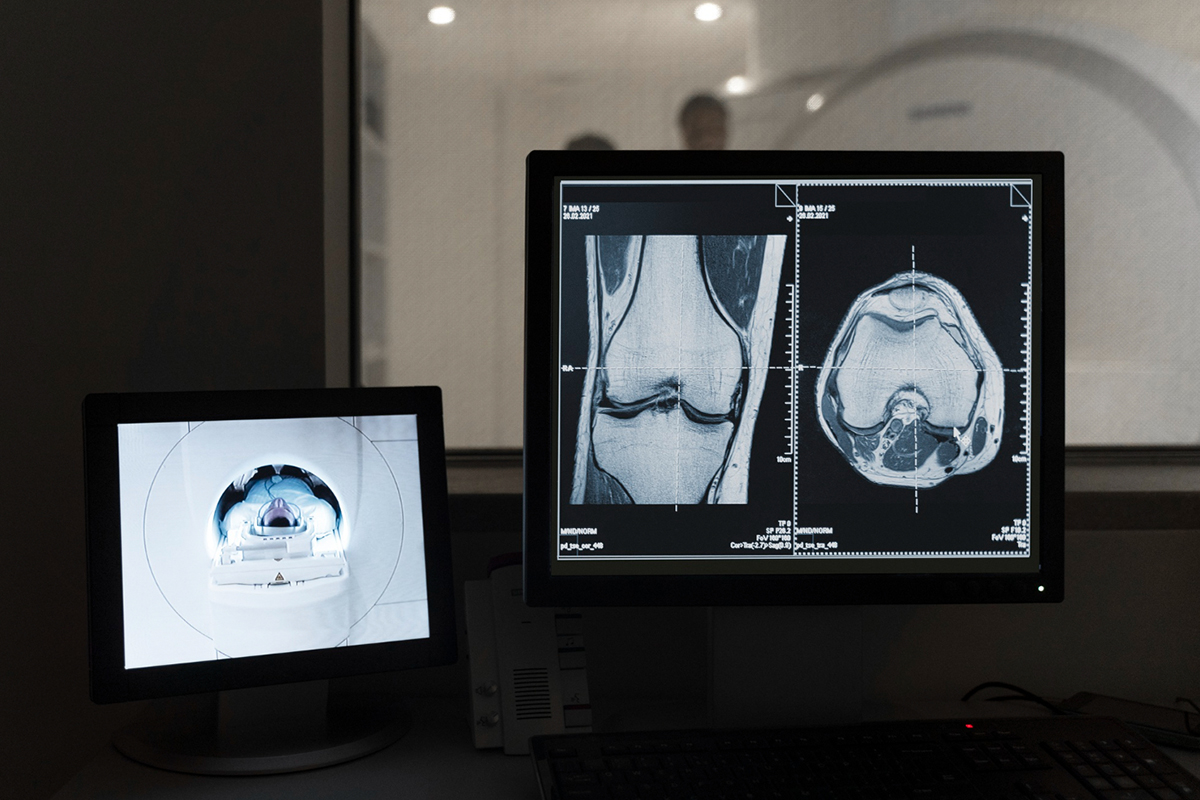
Magnetic Resonance Imaging (MRI)
-
Highly sensitive for early marrow involvement before bone destruction, critical for spinal metastases and soft tissue evaluation.

Positron Emission Tomography (PET)
-
Combined with CT, detects metabolically active tumors using 18F-FDG or 18F-NaF tracers, helpful for staging and treatment response.

Laboratory Tests
-
May show elevated serum calcium, alkaline phosphatase, anemia, or other tumor markers.
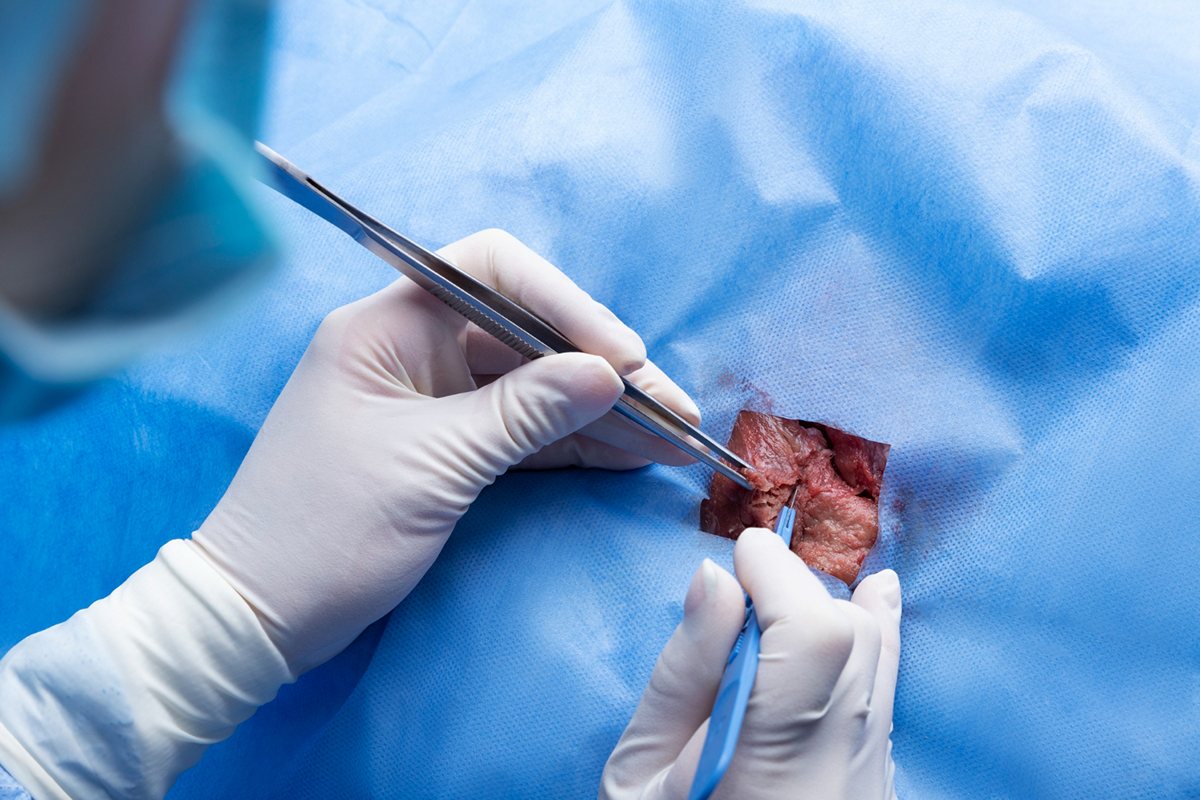
Biopsy
-
Definitive diagnosis by sampling bone lesion tissue via CT or MRI-guided core needle biopsy to confirm metastasis and identify primary tumor origin, especially when unknown.